The Bathroom Breaks Every Fall Detection System — Here's What We Built Instead
The first thing I noticed, walking a memory-care wing after the night shift had settled, was the pendant on the vanity.
It was clipped to its charger, blinking patiently, exactly where the resident had left it before bed. The whole multi-thousand-dollar promise of personal emergency response — press the button, help comes — was sitting in the bathroom, three feet from the most dangerous floor in the building, doing nothing. The resident was asleep. When she got up at 2 AM to use that bathroom, she would walk past her safety device to get there.
That image is most of what's wrong with fall detection in senior living, and it took me a long time to understand why. We build for the moment of the fall. The whole industry does. But the resident who is going to fall is not thinking about your device, can't reach it, and in the worst cases can't even remember she owns it. The technology that protects her has to require nothing from her at all. That is a much harder problem than "detect a fall," and it's the one we ended up building Veriprajna's smart facility fall detection system to solve — passive sensing that covers the rooms where falls are most dangerous and the residents least able to call for help.
Let me tell you how I got there, including the bet I made early that was wrong.
The Three Options That All Fail at 2 AM
When a facility administrator asks "what are our options for fall detection," there are essentially three answers on the market, and all three break at the exact moment they're supposed to work.
The first is the wearable pendant — the personal emergency response system, or PERS. It assumes an eighty-five-year-old with mild cognitive impairment will remember to wear it, keep it charged, and press it mid-crisis. The adherence data is brutal: 24% of PERS users never wear the pendant at all, only 14% achieve genuine round-the-clock adherence, and 30% abandon the device within six months. It comes off for bathing, for sleeping, for charging — and the bathroom, where it comes off, is the highest-risk room in the building.
The second is the camera. AI camera systems like SafelyYou produce genuinely strong clinical results — 40% fewer falls and 80% fewer fall-related ER visits in their deployments. I have real respect for that evidence. But a camera cannot go where it matters most. Nineteen states now regulate cameras in nursing-home rooms, up from nine in 2020, and bathrooms are categorically off-limits everywhere. State survey agencies have started citing facilities for "surveillance without consent." A camera that watches the bedroom but not the bathroom is covering the second-most-dangerous room while leaving the first one dark.
The third is the bed alarm — pressure mats and exit sensors. These detect bed exit, not falls. They tell you the resident left the bed. They do not tell you she fell on the way to the bathroom thirteen seconds later. And they fire constantly: a typical deployment throws five to fifteen false alarms per room per day.
Alarm fatigue is the number-one reason facilities abandon fall-detection technology. When every alert sounds the same, none of them mean anything.
That last sentence is the one I'd underline. Alarm fatigue isn't a UX annoyance — it's the failure mode that kills the whole category. I've watched it happen, and I'll come back to it, because I caused a version of it myself.
The Long Lie Is the Thing Nobody Costs Correctly
The part of this problem I didn't appreciate until I was deep in the clinical literature is that the fall is often not what kills you. The time on the floor is.
If an older adult is on the ground for more than an hour, half of them are dead within six months — even when the fall itself caused no serious injury. The body doesn't tolerate lying immobilized on a tile floor. Rhabdomyolysis shows up in well over half of fall cases involving immobilization; then come hypothermia, dehydration, pressure injury, acute kidney failure. Twenty percent of elderly fall patients who reach the emergency department had been on the ground more than an hour.
Now overlay the staffing reality. 63% of assisted-living facilities are short-staffed, 87% report difficulty hiring, and night-shift ratios that average one caregiver to fifteen residents stretch to one-to-twenty in poorly staffed buildings. Turnover runs 70–80% within the first hundred days. The CMS nursing-home staffing mandate was repealed at the end of 2025 precisely because the workforce to meet it doesn't exist.
So picture the 2 AM scenario that every one of these buildings is one bad night away from. A resident gets out of bed. The pendant is on the nightstand. A bed alarm fires, and a CNA mid-way through a med pass on the opposite wing taps to acknowledge it. The resident walks to the bathroom, catches a foot on the bath mat, and goes down hard onto the tile. She can't reach the pull cord. She can't get up. Without a sensor in that room, she is found at the 4 AM round. That is a hundred-plus-minute long lie, and it carries that 50% six-month mortality risk.
The cost shows up everywhere. A single fall with injury averages $30,000 in hospital and downstream care; falls cost the U.S. roughly $19.8 billion a year. And the liability is its own category — I've read negligent-monitoring settlement summaries running from the high six figures to $1.7 million for a single subdural-hematoma-plus-hip-fracture case. The claims are increasingly built on a specific argument: the prevention technology existed, and you didn't deploy it.
I Bet on Wi-Fi. The Building Said No.
Here's where I got it wrong, and I backed the wrong call with conviction.
When I first scoped this, I fell in love with Wi-Fi sensing. The pitch is irresistible: the radio signals already flooding every room shift subtly when a body moves through them, and you can read those shifts — channel state information — to detect motion and even falls. No new hardware in the room. No cameras, no wearables. Whole-building coverage from infrastructure that's already there. And the timing felt perfect — the IEEE 802.11bf WLAN-sensing standard was ratified in September 2025, which everyone read as the starting gun for sensing-enabled Wi-Fi. I argued, internally and hard, that this was the elegant answer: skip the per-room sensors, light up the whole facility with the access points it already owned.
Then we pulled a real facility's access-point inventory and the elegant answer died on a spreadsheet.
The standard being ratified does not mean a building's ten-year-old access points can expose channel state. Most of them can't — they don't surface the data, there's no VLAN segmentation to carry it cleanly, and the radios predate the entire idea of sensing. The infrastructure-readiness gap between "the standard exists" and "you have working fall detection" turned out to be the whole project. Around the same time, Verizon announced it was shutting down its Origin-Wireless-powered Home Awareness service on April 15, 2026 — the most visible consumer Wi-Fi-sensing channel, gone. That wasn't a coincidence I could wave away. It was the market telling me the same thing the spreadsheet did: this modality is real, but it is not ready to carry the rooms where a missed fall kills someone.
The standard being ratified is not the same as your building being ready. The deployment gap between those two facts is where every Wi-Fi-sensing pilot quietly dies.
That failure cost us time, and it cost me the satisfaction of the clean single-technology story. But it bought the insight the whole product now rests on: there is no one sensor. There's a modality that fits each room, and the engineering is in choosing correctly and stitching them together.
The one thing the spreadsheet did change for good: now, whenever a facility is already cutting a check to upgrade its Wi-Fi — and most are, with senior-living tech budgets up 6–30% year over year and two-thirds of operators pouring money into high-speed internet — I tell their IT lead to spec sensing-capable, 802.11bf-ready access points on that same purchase order. The standard finally exists. The cheapest sensing coverage you will ever buy is the radio you were already replacing.
Why Does Radar Win the Bathroom?
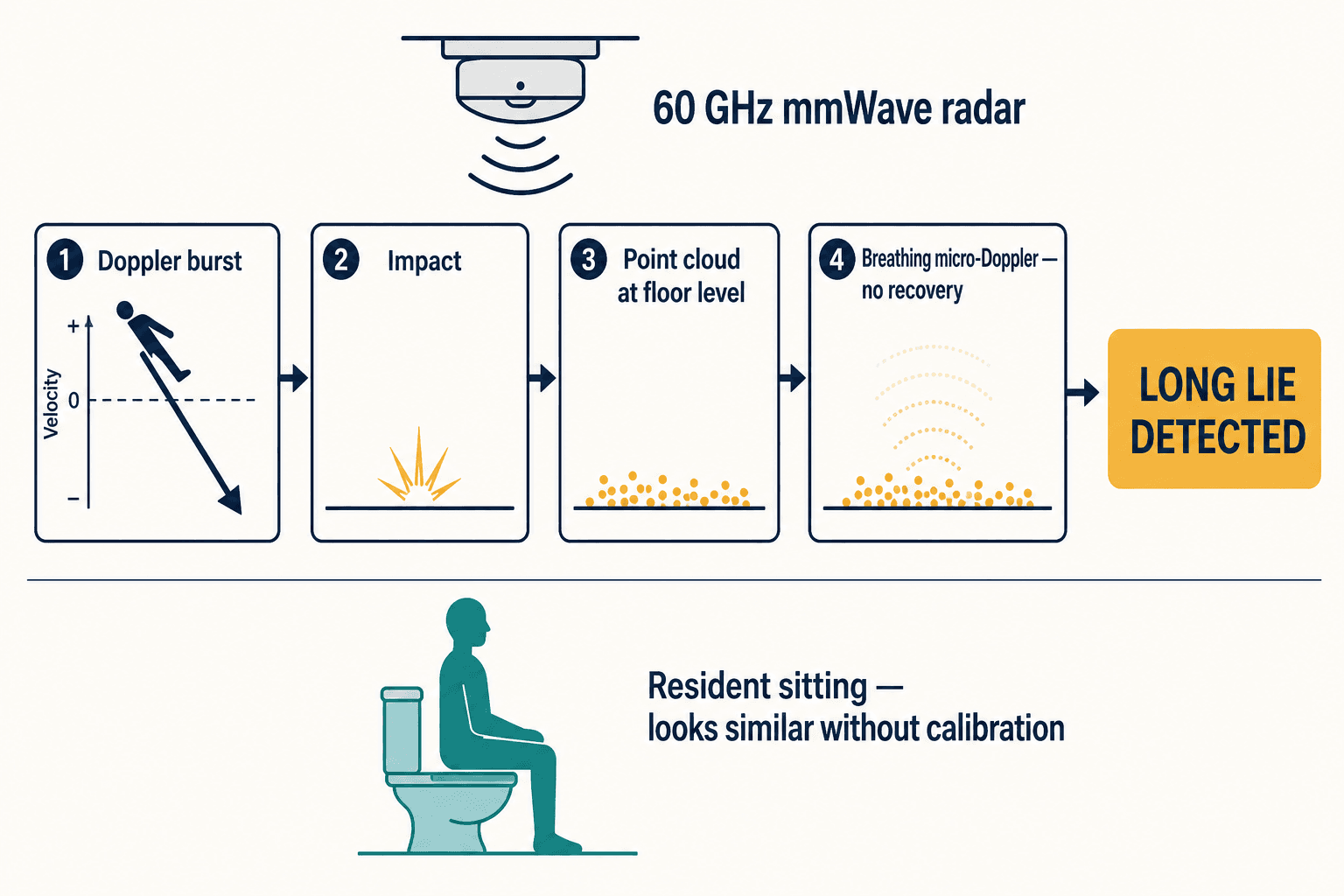
For the bathroom — the room no camera can enter and no pendant survives — the answer is 60 GHz millimeter-wave radar. A small module on the ceiling emits radio waves and reads what bounces back, building a four-dimensional picture: range, velocity, and angle, refreshed many times a second. It sees through a shower curtain. It works in total darkness. It produces no image, so there's no privacy objection and no camera-law problem — to a regulator, radar output is anonymous motion data, not personally identifiable information.
But one expert detail separates a system that works from one that gets muted by week three. A real fall has a signature. The radar sees a sudden Doppler burst — the velocity spike of a body going down — then an impact, then a point cloud that settles at floor level. And then it watches for what comes next: micro-Doppler from the chest, the tiny periodic motion of breathing, with no gross-motor recovery. That combination — on the floor, still breathing, not getting up — is the long lie. It is also exactly what a generic radar model trained on open bedrooms gets wrong, because a person sitting quietly on the toilet looks alarmingly similar if you haven't calibrated for that room's geometry.
I learned that the hard way too. In an early radar pilot we leaned on a vendor's off-the-shelf model, and in the bathroom it kept firing — on residents who had simply sat down. I watched a nurse, after the fourth or fifth false alarm in a shift, reach over and turn the volume down. That's the moment the whole investment becomes worthless. I had recreated the exact alarm fatigue I'd spent months telling administrators we would solve, and I'd done it by treating a sensor as plug-and-play. False-alarm reduction in a bathroom is not a setting you toggle. It's environment-specific calibration — the room's fixtures, the resident's mobility profile, the difference between a transfer and a collapse — and almost no vendor solves it for your actual rooms.
The commercial radar landscape is real and maturing. Vayyar's 4D imaging radar is running in one of the largest single fall-detection installations in the UK and has cut hospital admissions and long lies. Milesight's VS373 claims a 99% fall-capture rate with under 5% false alarms. Asahi Kasei is putting a 23-millimeter radar module into mass production this spring. The hardware is not the bottleneck. The bottleneck is that each of these is a proprietary stack, calibrated generically, costing $150–400 per room, and none of them tells you which rooms actually need it.
So Where Does Wi-Fi Belong?
Not in the trash — in the hallways and common areas, where the stakes per event are lower and whole-building coverage is the point. This is the multi-modality strategy nobody on the vendor side will sell you, because every vendor sells one thing.
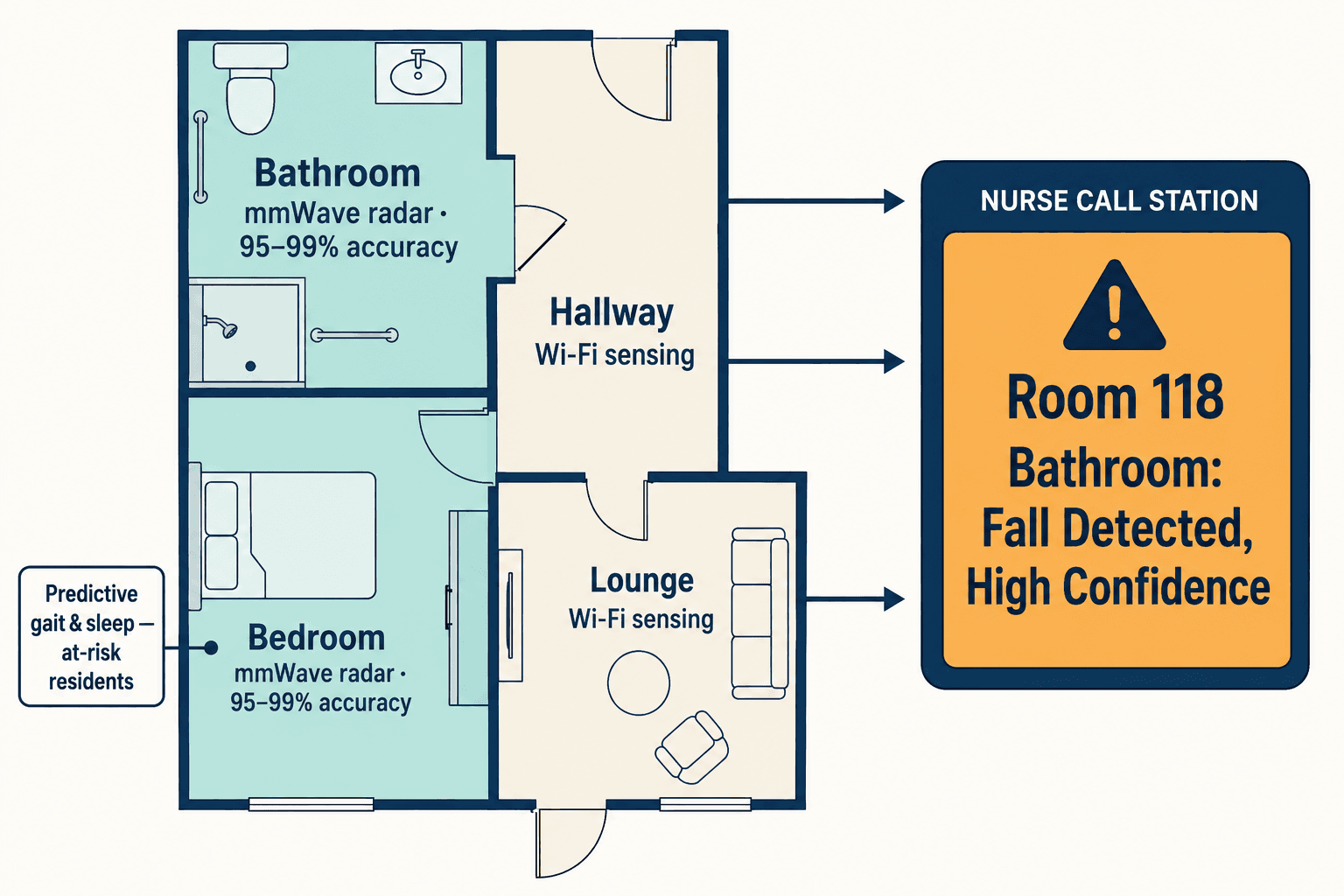
Put radar in the bathrooms and the high-risk bedrooms, where 95–99% accuracy and bathroom-safe coverage justify a dedicated sensor. Wi-Fi sensing then earns its keep in the corridors and lounges — where a per-room sensor budget could never reach, and where the building's infrastructure can actually support it. And for the residents who warrant it, the predictive layer comes in earlier still: systems like Helpany's "Paul" monitor gait and sleep to flag rising fall risk three weeks before an incident, and have delivered an average 66% fall reduction across fourteen Arizona communities. VirtuSense's infrared predicts bed and chair exit thirty to sixty-five seconds ahead. Each modality has a job. The consulting decision — which technology in which room, against this building's budget, layout, and wiring — is the part that determines whether any of it works.
That's the modality-agnostic stance we ended up taking, and it's genuinely uncomfortable as a business model, because it means we'll tell a facility not to buy radar for a hallway. But it's the only honest answer to a problem where the right sensor is different in every room.
Why Is the Nurse Call the Real Project?
If I could put one sentence in front of every administrator evaluating this technology, it's this: the sensor is the easy part.
A radar module that detects a fall with 99% accuracy is worthless if its verdict doesn't reach a human in time. The actual deliverable is a line on the nurse-call station that reads "Room 118 Bathroom: Fall Detected, High Confidence, Resident on Floor" — fast, trustworthy, and routed to the right caregiver. Getting there means integrating a sensor's output with the facility's existing nurse-call head-end — Rauland, Ascom, Austco, Hill-Rom — and that is deep systems-integration work, not an API key. In every real deployment I've costed, the integration and calibration is where the majority of the budget and effort actually goes. Vayyar has built some nurse-call partnerships, but implementation still varies facility to facility, because every building's wiring and workflow is its own snowflake.
Buyers think they're buying a sensor. What they actually need is a verdict that a tired CNA at 2 AM will trust and act on. That's an integration problem, not a hardware spec.
This is also why the off-the-shelf-versus-custom distinction matters so much here. The sensors are commodities trending toward zero. The value is in the unglamorous middle: tuning the model to these rooms so it stops crying wolf, and wiring the alert into this nurse-call system so it lands where someone can act on it.
The Objections I Hear Every Time
People always ask whether the regulatory case actually pushes toward this, or just permits it. It pushes. CMS's F689 standard requires facilities to be free of accident hazards with adequate supervision, and the agency tightened its fall-with-major-injury quality measure in 2025. Under the PDPM payment model, preventing falls and rehospitalizations directly protects reimbursement. And as cameras draw more state restrictions every year, the regulatory current is running toward exactly the non-camera, privacy-preserving approaches radar and Wi-Fi sensing represent.
The other question is always money, and I understand the reflex — tech budgets in senior living are real but not infinite, even as operators raise them 6–30% year over year. The number that ends the argument is the ROI: evidence-based fall-prevention programs return about $5 for every $1 spent. Against a $30,000 average cost per injurious fall and seven-figure liability exposure, the sensor-and-integration cost stops looking like a purchase and starts looking like insurance you actually collect on.
And occasionally someone asks whether this is just surveillance by another name. It's the opposite. A camera records you. Radar records that a body-shaped point cloud is at floor level and still breathing. The entire design goal is to know that someone needs help without knowing anything else about them — to protect the resident in the bathroom precisely by not being able to watch her there.
What I'd Tell the Administrator Now
The pendant on the vanity is still the image I come back to. We spent years building technology that asks the most vulnerable person in the building to participate in her own rescue, and then we're surprised when she can't. The shift that matters isn't a better sensor. It's accepting that the protection has to be ambient — in the room, requiring nothing of her at all.
That's what we built, and the hard-won lesson underneath it is that no single technology gets you there. Radar owns the bathroom. Wi-Fi covers the hallways your budget can't. Prediction flags the resident before the night she falls. And the integration into your nurse-call system — the part everyone treats as an afterthought — is the part that decides whether any sensor's alert reaches a human before the hour on the floor that turns a scare into a six-month mortality risk. If you want to see how those pieces fit a real building, that's the system we laid out.
The bathroom is the hardest room in senior living to protect, and it's the one that matters most. Any fall-detection plan that leaves it dark has solved the easy half of the problem and called it done.